Search

Delivering the National Cancer Plan
Why the National Cancer Plan raises a delivery challenge
England’s National Cancer Plan sets out renewed ambitions to improve cancer survival through earlier diagnosis, expanded screening programmes and faster diagnostic pathways. Independent analysis shows that 62 day performance would need to improve around 30 times faster than the current rate to meet national cancer standards, highlighting the scale of the challenge.[1]
National policy commits to expanding diagnostic infrastructure, including Community Diagnostic Centres (CDCs), wider use of digital tools and full rollout of lung cancer screening by 2030. As screening expands, downstream diagnostic services will require sufficient reporting, specialist assessment and workforce capacity to keep pathways moving.
To understand these pressures, Xyla convened a roundtable of clinical leaders, commissioners and community partners. Their insights, combined with Xyla’s operational experience, including reviewing more than 40,000 lung cancer screening report scans and enabling 48% of dermatology referrals to be managed safely in primary care, inform this briefing. It outlines where pressure is greatest across diagnostic and screening pathways and highlights the operational actions most likely to strengthen pathway performance.
Table of Contents

Where cancer pathways are currently under the greatest pressure
Imaging: Reporting turnaround increasingly determines pathway speed
Imaging remains one of the most constrained parts of the cancer pathway.
In 2024:
Across many systems, delays occur between scan completion and clinical reporting, slowing staging decisions and MDT discussions. Many rely on CDCs to expand imaging capacity, but sustaining extended CDC operating hours requires sufficient workforce, reporting capacity and clear escalation pathways into specialist assessment.
Where reporting turnaround is protected, pathway flow improves. This is illustrated in lung cancer screening programmes delivered by Xyla, where protecting reporting processes enabled more than 40,000 scaned reports to be reviewed within defined timeframes, allowing patients needing further investigation to be escalated rapidly.
Some services are exploring AI‑assisted reporting and automation to support diagnostic services. While still developing, these tools may help increase reporting efficiency when combined with appropriate clinical oversight.
Key learning: Reporting capacity increasingly limits pathway speed.
Systems may need to prioritise protected reporting time and strengthen escalation routes to maintain diagnostic flow .

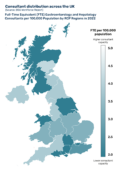
Endoscopy: Workforce pressures limit expansion
Endoscopy services continue to experience sustained workforce pressure.
Gastroenterology has the largest medical waiting list, with:
These pressures make it difficult to expand diagnostic capacity as demand grows. Persistent shortages also limit the ability to extend operating hours or reliably staff additional lists.
Operational experience shows that pathway flow improves when recovery, histopathology and follow‑up capacity are aligned. In one endoscopy programme supported by Xyla, more than 2,900 procedures were delivered through extended sessions where downstream capacity was coordinated effectively, helping maintain flow despite workforce pressure.
Key learning: Workforce flexibility is essential to expanding diagnostic capacity.
Flexible staffing models and aligned recovery and histopathology capacity can sustain activity even when workforce constraints persist.
Breast services: Screening expansion increasing downstream demand
Breast screening continues to expand and plays an important role in earlier cancer detection.
In 2024/25:
1.94 m
women were screened within six months of invitation, almost 200,000 more than the previous year [5]
While this expansion supports earlier diagnosis, rising participation places additional pressure on radiology, pathology and surgical clinics. Sustained performance depends on diagnostic reporting and specialist assessment keeping pace with increased imaging activity.
In breast diagnostic services supported by Xyla, extended imaging sessions increased one‑stop clinic capacity and enabled faster assessment for two‑week‑wait patients, contributing to shorter waits and reduced local backlogs.
“What we are seeing is that the expansion of screening is reshaping patient flow as much as it is increasing volume. Earlier detection creates real opportunity, but only if diagnostic and specialist capacity can scale in step. Without that alignment, pressure is not removed, it is displaced further along the pathway, ultimately presenting as longer waits and delayed treatment for patients.”
Nicola Ellis-Webb, Healthcare Services Director, Xyla
Key learning: Workforce capacity must scale with screening demand.
Screening growth translates into earlier diagnosis only when reporting and specialist clinic capacity expand alongside imaging activity.

Find out more about how a large acute hospital partnered with Xyla to increase weekend capacity within its one-stop breast clinic.
Read moreDermatology: Rising demand across skin cancer pathways
Dermatology demand continues to grow rapidly, placing sustained pressure on skin cancer pathways.
As diagnostic demand grows, many systems are adopting digital approaches to improve referral quality, prioritise urgent cases and increase pathway visibility. Digital triage combined with rapid remote specialist review helps ensure urgent referrals are identified quickly while reducing unnecessary escalation to secondary care.
Experience from Xyla’s teledermatology service shows how early consultant input can ease demand. Rapid review has strengthened triage, reduced pressure on urgent pathways and enabled 48% of referrals to be managed safely in primary care, easing pressure on two‑week wait clinics.
Key learning: Data visibility determines whether pathways flow or stall.
Integrated booking and reporting tools provide real time oversight of pathway activity and help reduce hidden delays between referral, testing and escalation.
Key learning: Referral quality matters as much as referral volume.
Digital triage and early consultant review help ensure urgent two‑week‑wait capacity is focused on those who need it most.
“A patient referred as urgent had a high-risk nodular melanoma. Without photo triage they may have waited months. With rapid imaging and virtual review, they will now receive treatment within two weeks, which could make all the difference.”
Xyla Consultant Dermatologist, Frimley ICB

Cancer screening uptake across NHS programmes
Screening uptake varies significantly between regions
Uptake is lowest in more deprived communities, where transport, language, digital exclusion and health literacy barriers affect participation. Community‑based engagement and flexible access models can help address this. In lung cancer screening, mobile teams supported by Xyla increased uptake among groups less likely to engage, including a 10% rise among previous non-responders.
A key barrier is the siloed delivery of breast, bowel and cervical screening, which targets similar age groups but operates separately, duplicating effort and cost. In Xyla’s lung cancer screening programme, engagement accounted for around 25% of total spend, showing how coordinated outreach could use resource more efficiently.
A more joined up approach, such as offering bowel screening kits during lung checks or aligning breast and cervical messaging, would reduce duplication and improve uptake in underserved groups.
Key learning: Improving participation requires different delivery models.
Community outreach and flexible access models increase uptake when paired with sufficient downstream diagnostic capacity.

A readiness framework for the National Cancer Plan
Delivering the ambitions of the National Cancer Plan will depend on how effectively systems align diagnostic capacity, workforce and digital infrastructure. The questions below are designed to help leaders assess where pathways are strong and where further focus may be needed.
Workforce capability
- Which diagnostic workforce groups are most likely to limit pathway delivery in the next 3 to 5 years?
- Do teams have the flexibility to deploy staff across sites and sessions where pressure is highest?
- Do you have access to sufficient capacity, either internally or through partnership working?
Diagnostic capacity and pathway performance
- Where are the most significant diagnostic bottlenecks and how consistently are scan‑to‑report times achieved?
- Is current reporting and escalation capacity sufficient to support earlier diagnosis and faster assessment?
- Are recovery, pathology and follow‑up steps aligned to prevent downstream delays?
Screening expansion
- Is the system ready for full rollout of lung cancer screening and the associated diagnostic demand?
- Are reporting and specialist clinic capacity increasing at the same pace as screening participation?
- How will services ensure that increased screening translates into timely diagnosis rather than additional backlog?
Data and digital infrastructure
- Do teams have real‑time visibility of diagnostic flow, delays and escalation points?
- Are booking, triage and reporting systems integrated enough to support coordinated pathways?
- Can digital tools, such as remote review, reduce avoidable pressure on face‑to‑face services?
Equity and access
- Do teams understand screening uptake and access barriers in detail across different population groups?
- Are targeted engagement approaches in place where participation is lowest?
- Is downstream capacity sufficient to meet increased demand if uptake improves?
Partnerships and external capacity
- Can external partners be integrated rapidly into governance and pathways when capacity gaps emerge?
- Are contracts structured to flex capacity up or down as demand changes?
- Is there clarity on where external support provides greatest value and where it could reduce risk?
Supporting local delivery of the National Cancer Plan
The National Cancer Plan sets an ambitious direction for improving cancer outcomes through earlier diagnosis, expanded screening and faster diagnostic pathways. For many systems, the immediate challenge will be ensuring that diagnostic pathways are configured to translate increased activity into faster diagnosis and treatment.
The insights in this briefing are intended to support local leaders in identifying where operational pressures are most likely to affect pathway performance and where targeted action may have the greatest impact.
Xyla works with NHS organisations across diagnostic and screening services, including lung cancer screening, breast diagnostics, teledermatology and endoscopy support.
For further information get in touch:
Fields marked with an * are required.
If you’d like to download this briefing, you can do so here. Please feel free to share it with your colleagues and wider networks.
Download PDF versionReferences:
[1] https://www.nuffieldtrust.org.uk/news-item/nuffield-trust-response-to-cancer-target-announcements
[4] https://pubmed.ncbi.nlm.nih.gov/36818791
[6] https://cdn.bad.org.uk/uploads/2024/09/10155802/BAD-Workforce-Census-Report-Sept-24.pdf
[7] https://gettingitrightfirsttime.co.uk/wp-content/uploads/2021/09/DermatologyReport-Sept21o.pdf
[8] https://www.england.nhs.uk/2025/02/record-breast-screening-level

Related Stories



Share this article

Contact us
Have any questions about our services? Whether you’re wondering about how we can help your health goals, or assist your healthcare organisation, we’d love to hear from you.
Get in touch